Observations
Over the last 12 months, RightShip has reviewed the close out reports for over
- 700 PSC detentions
- 2400 incidents
which have occurred within this period.
In each case, the close out report provided by the technical managers of the vessel included a section titled root cause, however the majority of reports incorrectly labelled an immediate cause / causal factor or an intermediate cause as a root cause and did not identify more than one cause.
An immediate cause or a causal factor is a cause that directly resulted in the unplanned adverse event or allowed the consequences to be worse than they might have been, and if eliminated or modified, would have prevented the undesired outcome. An immediate cause is mostly associated with unsafe acts, unsafe conditions or both, and for a typical incident there are multiple immediate causes or causal factors.
An intermediate cause is “an underlying reason why a causal factor occurred, but it is not deep enough to be a root cause” (ABS, 2005).
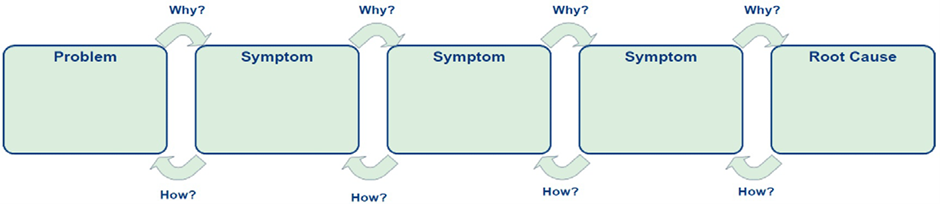
A root cause is a failure of the ‘management system that allows the causal factors to occur or exist’ (ABS, 2005). It can also be defined as “the most basic cause or causes that can reasonably be identified and that management has control to fix, and when fixed will prevent or significantly reduce the likelihood of the problem’s recurrence” (TapRooT, 2016). The terms associated with incident investigations are shown in Figure 1.

Figure 1: Relationship of Incident Investigation Terms (Adapted from ABS, 2005)
The definition of root cause highlights that unless the underlying and most basic causes of the problem are identified, vessel managers will not find how to fix the problem. By stopping the investigation at the immediate or intermediate cause level, only corrective actions for that specific issue can be discovered. However, continuing the investigation to identify the root causes will allow effective preventive measures to be developed, and if these are implemented both the specific issue and the wider problem that may cause similar incidents to occur will be addressed.
This is why RightShip continues to ask vessel managers to identify the root causes, to prevent similar adverse events happening again for that vessel manager. A typical Request For Information (RFI) sent by RightShip to vessel managers is shown in Figure 2.

Figure 2: Example of Request For Information (RFI) sent by RightShip to Vessel Managers
It is also important to recognise that “there is very rarely one cause for an incident. “… Multiple safeguards exist to prevent or mitigate almost any incident worth investigating. Therefore, numerous failures of these safeguards have to occur to generate an incident” (ABS, 2005). For this reason, vessel managers that list a single cause for an adverse event miss the opportunity to identify all the remaining significant contributing factors.
Examples of poor root causes
What good Managers do
There are a number of different techniques that can assist in finding root causes, and even for creating effective preventive actions associated with the root causes. Using these tools will assist to systematically identify all causal factors, intermediate causes and underlying root causes associated with an adverse event. The list of techniques below shows four examples that are in wide use in the maritime industry, but there are other valid techniques available in addition to those listed.
- Five Whys
- TapRooT
- ABS Marine Root Cause Analysis Map
- DNV-GL 2015, Marine Systematic Cause Analysis Technique
Vessel managers that work hard to avoid accidents re-occurring take ownership of each near miss and adverse event, and do not accept that there was nothing they could have done to stop the adverse event from happening. Taking ownership of the issue ensures they meet the requirements of the International Safety Management Code (ISM Code), as required under Section 9 Reports and analysis of non-conformities, accidents and hazardous occurrences.
Taking ownership of the adverse event and using a recognised technique to identify root causes also assists vessel managers to avoid the common traps, which include those described by ABS (2005), and shown below in Figure 3.
Trap 1 – Plant Problems
One common trap that prevents organisations from searching for root causes in the belief that “It just wore out; nothing lasts forever” or “It was just a bad part”. Rather than adopt such a thought process, such problems should be viewed as follows:
• Structural/machinery/equipment/outfitting inspections, testing and maintenance can prevent most failures.
• Bad parts could be identified as part of the quality assurance process.
• Something can always be done to prevent failures. It must be decided whether to take action to prevent the failures.
|
Trap 2 – Personnel Problems
Another common set of traps that prevents organisations from searching for root causes in the belief that “Nobody else would have made that mistake; he has never been one of our best personnel” or “The procedures are right and she received our standard training; she just goofed up”. Rather than adopt such a thought process, such problems should be viewed as follows:
• How did this person come to be hired?
• Were the procedures that the person used accurate?
• Was the training correct and sufficient and did the company verify that the training was understood?
• Has this person committed this error before?
• Was the error detected before with someone else and were effective actions taken to prevent its recurrence?
Often it is not the individual who needs correcting, it is the environment in which they work that needs changing.
|
Trap 3 – External Event Problems
Another common trap that prevents organisations from searching for root causes is the belief that “It was a natural phenomena event beyond our control”. It is true that an organisation cannot prevent weather from occurring or individuals from choosing to attempt to harm a vessel or its personnel, however, plans need to be in place for natural phenomena events and other external factors to minimise the consequences of these events when they do occur.
|
Figure 3: Root Cause Analysis Traps, (ABS 2005)
To assist in the identification of all causal factors, it is necessary to consider the hazard control aspects in terms of People / Process / Plant, by asking:
- How did the actions of the people, often referred to as work-as done (WAD), contribute to this event
- What gaps in procedures contributed to this event?
- What failures of machinery or equipment contributed to this event?
The identification of additional causal factors will lead to a greater understanding of the root causes and subsequently enhance the efficacy of preventive measures.
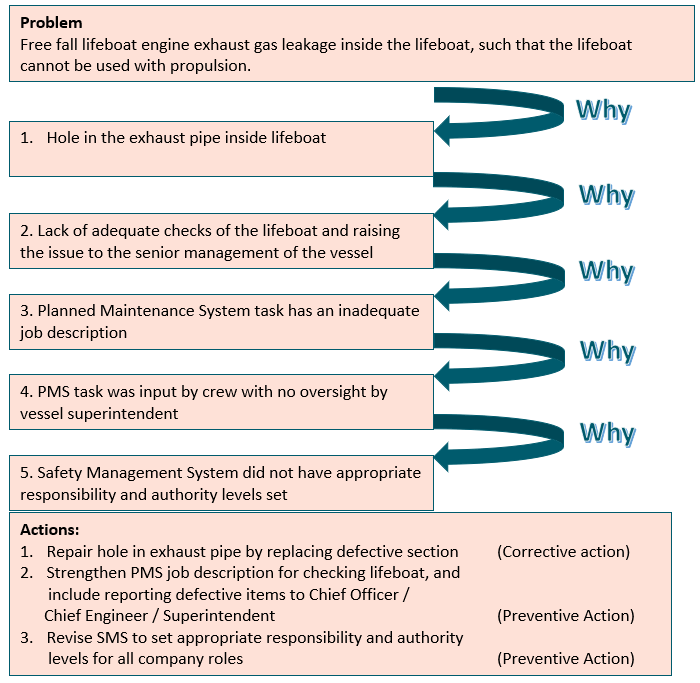
Example of Root Cause Analysis, using 5 Whys
The 5-Whys is a simple brainstorming tool that can help teams identify the root cause(s) of a problem. Asking the 5-Whys allows teams to move beyond obvious answers and reflect on less obvious explanations or causes.
Step-by-step instructions
1. State the problem you have identified as a strategic problem to work on.
2. Start asking “why” related to the problem. Keep asking why in response to each suggested cause.
3. Ask as many whys as you need to get insight at a level that can be addressed (asking five times is typical). You will know you have reached your final “why‟ because it does not make logical sense to ask why again.
Asking "Why?" five times successively, you can delve into a problem deeply enough to understand the ultimate root cause. By the time you get to the 4th or 5th why, you will likely be looking squarely at management practices (more than five whys may be required for complex problems).
At this point you understand the root cause and can see where a preventive action is needed.
The 5 Why Template
Example in use:
Summary
Every incident is avoidable, and Root Cause Analysis is an effective method for identifying underlying causes in the management system, to determine the actions necessary to correct the failures. Determine what adverse events have occurred. Then, examine the complex systems surrounding the problems and identify failure points. Determine solutions to address these critical issues, or fundamental causes. If you only address the identified deficiency, the problem will almost certainly recur, requiring you to address it again and again and again. If you look further to understand why the problem is occurring, you may correct the underlying systems and practises that are contributing to it.
How to execute:
1. Learn what happened.
2. Identify the fundamental reason.
3. Find out what needs to be done to reduce the likelihood that it will happen again, for all the vessels in the fleet.
People, Plant, and Processes are the three primary contributors to the root causes. Identify the maximum number of contributing factors. Too often, individuals stop after identifying only one or two factors, which is insufficient. With RCA, the analyst shall go beyond merely addressing the most obvious problems. Determine the necessary adjustments for each system by analysing the mechanism of cause and effect.
Planning in advance will assist you in anticipating the results of your solution. This allows for the identification of potential issues prior to their occurrence.
Truthfulness throughout the analysis will aid the organisation in correctly identifying the issue and identifying a solution.
Where to find further information
- Appendix 1 – The Root Cause Analysis Process, Original article sourced from Mind Tools Ltd.
http://www.mindtools.com/pages/article/newTMC_80.htm
- TapRooT® 2019, ‘Root Cause Analysis, Definition of a Root Cause’,
https://www.taproot.com/definition-of-a-root-cause
- American Bureau of Shipping (ABS) 2005, ‘Guidance Notes on The Investigation of Marine Incidents’,
https://ww2.eagle.org/content/dam/eagle/rules-and-guides/current/other/142_investigationofmarineincidents/ii_rca_guidance_e-feb14.pdf
- RightShip Inspection Ship Questionnaire (RISQ), Version 3, February 2023, p12
RightShip’s Inspection Questionnaire RISQ
- International Maritime Organisation 2018, International Safety Management code (ISM code) and Guidelines on the Implementation of the ISM Code, London
